

Panic Attacks Aren't About Fear. They're About Being Left.
Most panic treatment targets fear. But panic and fear run on separate systems in the brain, with different chemistry, different circuitry, and different jobs. Understanding which one is actually firing changes what kind of help works.

Most people describe a panic attack the same way. It felt like dying. Like the room was closing in. Like something terrible was about to happen. So we treat panic like a fear problem. We teach breathing exercises, we challenge catastrophic thoughts, we tell the nervous system "you are safe right now," and sometimes that helps.
But it doesn't always help. I think that's because we're answering the wrong question. Panic isn't your brain asking "am I in danger?" It's an alert. An old, loud signal whose entire job is to maintain connection, by telling you, urgently, that you are disconnected right now or convinced that disconnection is about to happen.
Two different alarm systems
Your brain has more than one way to sound an alarm, and they're not the same circuit doing the same job at different volumes.
FEAR is the system that responds to a predator, a car swerving into your lane, a hand on a hot stove (by the way when something is all caps it means it’s a label for a brain system, when it’s not it means it is labeling an emotional feeling). It runs through the amygdala, it's fast, and it's built for immediate physical threat. This is the system most anxiety treatment is designed to address.
PANIC is different, and researchers actually call it PANIC/GRIEF, because it's one system with two faces. It runs a separate route from FEAR, through deep midbrain structures up to the anterior cingulate cortex, and it isn't regulated by the same threat chemistry. It runs largely on your body's own opioid system, the same chemistry involved in bonding and the comfort of closeness. When that opioid supply drops, the alarm goes off.
PANIC/GRIEF is unusual among the seven basic emotion systems in that its name captures two distinct phases of feeling. When panic does not result in feeling secure in connection or attachment again, or we have given up hope of that happening, our system collapses into the other side of that coin: an experience of grief. Grief is what it feels like when connection is already lost. It's the helplessness, the pain of isolation, the collapse that comes when there's nothing left to do about it. The feelings of panic come before that. PANIC's job isn't to cause us to brace for danger. It's to sound the alarm loudly enough, and urgently enough, that connection gets restored before it's lost for good. A panic attack is your system raising every biological and emotional signal it has, fast, because as far as it's concerned, the only thing standing between you and that collapse is whether the alarm works.
This is the same pattern researchers have long described in young mammals separated from a caregiver. First an active, distressed protest: calling out, searching, trying to restore contact. Only later, if reconnection doesn't come, a collapse into something quieter and more despairing. Panic is the protest call. It exists to bring someone back, or to bring you back to yourself, before the despair sets in.
This is also why a panic attack so often doesn't match the size of whatever triggered it. You're not overreacting to a small thing or having symptoms out of nowhere. A fast, old part of your brain has registered that the helplessness of isolation might be coming, and it's throwing everything it has at preventing that outcome, before you've even had time to name what's happening.
What "disconnection" actually means here
Surprisingly, the PANIC/GRIEF system doesn't only fire when someone physically leaves the room. It fires on a prediction (remember, the brain is a prediction machine, as neuropsychoanalyst Mark Solms has argued), and what it's predicting is whether GRIEF is about to arrive.
Underneath every panic attack is a fast, mostly unconscious assessment running on three things at once. A memory of what that helpless, isolated collapse has felt like before. A prediction about whether it's about to happen again right now. And a read on both yourself and the other person: whether you can survive being without them, whether they're still actually with you, whether this is the moment you finally fall into that state you already know.
That's why panic can show up in places that have nothing to do with relationships on the surface. A work presentation. A crowded store. A plane. What's actually being evaluated underneath isn't your presenting skills, the room, or the plane. It's closer to: "if this goes badly, will I end up alone with no way to fix it, and has that helplessness happened to me before?" If your history has taught your nervous system what that collapse feels like, your brain doesn't wait for it to arrive. It panics early, trying to head it off, because heading it off is the whole point of the system.
What's happening in your body
This system has a different chemical signature than fear does, and that's part of why fear-based treatment doesn't always land.
Where the FEAR system runs largely on CRF, norepinephrine, and the threat-detection chemistry of the amygdala, the PANIC/GRIEF system runs primarily on the brain's own opioids, along with oxytocin and prolactin, the same chemicals involved in bonding and the comfort of closeness. In animal studies, giving opioids is the single most effective way to quiet a separated infant's distress calls. That tells you what the alarm is actually built to respond to. Not threat reduction. Reconnection. It goes off when that opioid-driven sense of closeness drops, and it shuts off when closeness is restored, not when danger passes.
Here's the piece that explains what a panic attack actually feels like in the body. This circuit doesn't stop at producing an emotional signal. It directly regulates breathing, heart rate, and pain sensitivity as part of its basic function, and its territory overlaps with structures that also drive the body's fear and arousal chemistry, including norepinephrine. So when this alarm fires, it doesn't stay contained to "I feel disconnected." It recruits your sympathetic nervous system, the same system responsible for fight-or-flight, and that's where the racing heart, the shallow breathing, the sweating, and the trembling come from. The alert has to be loud enough, physically, to actually move you or someone else to act. A quiet signal doesn't restore connection. A racing heart and a flood of adrenaline-like chemistry does, because it's built to be impossible to ignore.
This is also why a panic attack can feel indistinguishable from a heart attack or a respiratory emergency. It isn't your imagination and it isn't "just anxiety." Your sympathetic nervous system has activated for real, your heart rate has climbed for real, your breathing has changed for real. The alarm is bodily because it has to be. A signal whose entire purpose is to summon connection back doesn't work if it's subtle.
The old proof: two problems, two drugs
Long before anyone had mapped this circuitry, clinicians stumbled onto evidence that panic and anxiety are actually two different problems, by accident, through a drug that only fixed one of them.
In 1960, a psychiatrist named Donald Klein was working at Hillside Hospital in Queens, New York, treating patients with severe anxiety attacks and agoraphobia. He was testing imipramine, one of the first antidepressants, which had only been introduced a few years earlier. What he found surprised him. Imipramine stopped the panic attacks themselves, often within weeks. But it didn't touch something else these patients were still carrying: the fear of having another attack. That anticipatory dread, and the avoidance behavior built around it, the not going to the store, the not getting on the plane, stuck around long after the attacks had stopped. It took a different kind of medication, an anti-anxiety drug, to work on that part.
Klein published this finding in 1962, and he called his method "pharmacological dissection." The logic was simple. If one drug stops the attacks and a different drug is needed for the fear of the attacks, you're probably not looking at one problem with two symptoms. You're looking at two different mechanisms that happen to sit next to each other. That observation eventually helped separate panic disorder from generalized anxiety disorder in psychiatric diagnosis, decades before anyone could point to the separate neurochemistry behind it.
It's a striking piece of history to sit next to everything above. Clinicians noticed, just from watching patients respond to medication, that panic and anxiety about panic were not the same thing and did not resolve through the same channel. That's the same split this whole piece has been describing, just discovered from the outside in, one prescription at a time, instead of from the inside out through brain circuitry.
Why this changes what helps
If panic is fundamentally a fear response, the treatment is exposure and reassurance. Prove to your nervous system that the room is not, in fact, dangerous.
If panic is fundamentally an attempt to maintain connection, the treatment has to focus on that. It's not enough to convince your nervous system that the plane won't crash, and it's not enough to slow the breathing once the sympathetic nervous system has already taken over, although that can help in the moment. The deeper work has two parts. One is with the prediction itself: what your body believes will happen, and what memory that belief is built on. The other is with your capacity to actually tolerate the thing panic is working so hard to avoid. As long as grief feels unsurvivable, the system has every reason to keep sounding the alarm rather than risk falling into it. Part of the work is building enough safety and support that helplessness and isolation, if they do show up, are no longer the catastrophe your body believes them to be.
This is part of why somatic and trauma informed approaches often reach panic in a way that pure cognitive reassurance doesn't. You can't think your way out of a prediction your body learned before you had words for it, and you can't think your way into trusting that grief, if it comes, is survivable. That trust tends to get built through relationship, through the body, through slowly proving to your nervous system, in small doses, that the helplessness it's so afraid of isn't the end of you.
The question underneath the question
If you've had a panic attack and wondered why "you're safe" never really helped, this might be why. Your nervous system wasn't asking about safety from harm. It was trying, urgently, to keep you from falling into a helplessness it’s known before.
That's not a flaw in your wiring. It's an old, well-intentioned system working as hard as it can to keep you from a pain it has every reason to believe is coming, sometimes in situations where that pain was never actually on the way. Understanding that doesn't make the panic disappear. But it changes what you're treating. You're not just talking your body out of a false alarm. You're slowly teaching it that even if grief came, you wouldn't be as alone in it as it fears.
An important note: most current clinical guidelines still treat panic attacks as an exaggerated fear response centered on the amygdala. The separation based view laid out here is a real, published alternative within affective neuroscience, but not something every researcher or clinician would sign off on. I find it more clinically useful for a lot of what shows up in the room, but it is a minority position within panic disorder research specifically, even though the PANIC/GRIEF system itself is well established as distinct from FEAR in the broader affective neuroscience literature.
References Used for this: The distinction between the FEAR and PANIC/GRIEF systems, including their separate neuroanatomy (amygdala and dorsal periaqueductal gray for FEAR; anterior cingulate, bed nucleus of the stria terminalis, and periaqueductal gray for PANIC/GRIEF) and their different core chemistry (CRF and norepinephrine for FEAR; endogenous opioids, oxytocin, and prolactin for PANIC/GRIEF), comes from the affective neuroscience research tradition built by Jaak Panksepp. It's summarized well in a 2020 paper by Gianni Francesetti, Antonio Alcaro, and Michele Settanni, "Panic disorder: attack of fear or acute attack of solitude? Convergences between affective neuroscience and phenomenological-Gestalt perspective," published in Research in Psychotherapy: Psychopathology, Process and Outcome. The protest and despair pattern in separated young mammals draws on John Bowlby's attachment research. The role of the PANIC/GRIEF circuit in directly regulating breathing, heart rate, and pain sensitivity, and the finding that opioids are the most effective known way to quiet separation distress calls in animal studies, are also drawn from that same research tradition. The sympathetic nervous system's role in producing panic attack symptoms such as rapid heart rate, shallow breathing, and sweating is well established in the clinical panic disorder literature more broadly. The imipramine finding comes from Klein DF, Fink M, "Psychiatric reaction patterns to imipramine," American Journal of Psychiatry, 1962;119:432-438, with later work on benzodiazepines and anticipatory anxiety summarized in Zitrin, Woerner, and Klein, 1981. Mark Solms's work on the brain as a predictive system draws on his 2021 book The Hidden Spring: A Journey to the Source of Consciousness.
The Hidden Nature of Attachment Beliefs and Their Impact on Professional Success
For a company to thrive, it’s essential that team members feel seen, heard, and understood. By learning to recognize and address attachment beliefs, leaders can foster a more inclusive and supportive environment. This not only improves interpersonal relationships but also enhances productivity, creativity, and overall job satisfaction.

Attachment beliefs are like invisible forces shaping our behaviors, often without us realizing it. These beliefs were formed before the left side of our brain—the part responsible for logic and conscious thought—was fully developed. Instead, they’re rooted in the right side of the brain, where feelings dominate and conscious reasoning takes a backseat.
This makes attachment beliefs tricky to recognize and even harder to change. When we think about our attachment behaviors, it’s easy to focus on situations where we’re consciously aware of our choices and actions. However, to truly understand and work with attachment, we need to shift our focus to those moments when we don’t notice anything wrong at all.
Imagine being in a conflict where you’re utterly convinced of your perspective, yet others around you question your behavior. Their doubts might leave you feeling confused or even defensive because, in your mind, everything makes perfect sense. This disconnect happens because attachment beliefs operate on an unconscious level. They’re so deeply ingrained that they influence our actions and reactions without us being aware of it.
In a professional setting, these unconscious patterns can significantly impact team dynamics, communication, and overall company success. If left unchecked, attachment beliefs can lead to misunderstandings, hinder collaboration, and create an environment where employees may feel disconnected or undervalued.
Understanding this is key for leaders and team members alike. By becoming more aware of these unconscious patterns, we can start to see where our beliefs might be holding us back or causing misunderstandings in the workplace. This awareness is the first step in making changes that lead to healthier, more authentic connections with others.
For a company to thrive, it’s essential that team members feel seen, heard, and understood. By learning to recognize and address attachment beliefs, leaders can foster a more inclusive and supportive environment. This not only improves interpersonal relationships but also enhances productivity, creativity, and overall job satisfaction.
In the end, working with attachment beliefs isn’t about fixing what’s broken but about shining a light on what’s hidden. It’s about being open to the possibility that there’s more going on beneath the surface than we realize—and that by exploring these depths, we can unlock greater potential for both personal growth and professional success.
What Are Attachment Styles?
Attachment styles are ways people connect and relate to others based on their early experiences with caregivers…These patterns often continue into adulthood and influence romantic relationships. People tend to form relationships with partners who have similar attachment styles to one or both of their parents.
Attachment styles are ways people connect and relate to others based on their early experiences with caregivers. John Bowlby, a psychiatrist and psychoanalyst, developed Attachment Theory, sometimes called the science of love, after studying relationships between mothers and troubled teenagers. He wanted to understand how early relationships influenced later behavior. Along with his colleague Mary Ainsworth, who studied interactions between parents and young children, they identified different attachment styles based on how children responded to connection, separation, and reconnection with their caregivers.
Ainsworth's research led to the creation of "The Strange Situation," a study that helped categorize four main attachment styles.* These styles are learned behaviors developed in response to early experiences of distress and are not meant to label someone as good or bad. Instead, they show how a child felt they needed to behave to feel emotionally safe with their caregiver. These unconscious patterns often continue into adulthood and influence romantic relationships, parenting, friendships and professional life. People tend to form relationships with bosses, co-workers, friends and partners who have similar attachment styles to one or both of their parents.
The Four Attachment Styles
1. Secure Attachment
Children with secure attachment felt listened to and trusted that their feelings would be respected. They grow up with a healthy ability to handle emotions and feel good about themselves.
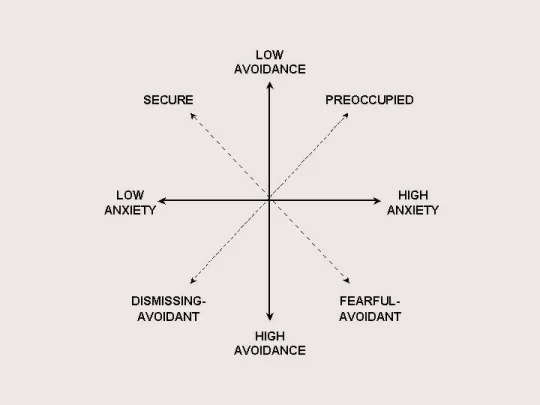
2. Anxious/Ambivalent (Preoccupied) Attachment
These children experienced inconsistent attention from their parents, leading to prolonged anxiety. They learned to keep their parents' attention by being pleasing or entertaining, but this created a sense of low trust and a need to control. As adults, they might seem clingy, angry, controlling, or critical, stemming from a deep fear of abandonment and insecurity. Often they have to dissociate negative emotions like anger for fear it would cost them the relationship.
3. Dismissive/Avoidant Attachment
Children with this attachment style learned that expressing big emotions would be ignored, so they turned down their anxiety and disconnected from their feelings. They often come off as self-sufficient, preferring solo activities over team or emotional ones. They might appear uninterested in close relationships, masking low self-esteem with an inflated sense of independence.
4. Anxious/Avoidant (Fearful Avoidant) Attachment
These children experienced both pain and comfort from their parents, often due to abusive relationships. They couldn't develop a stable coping strategy, leading to a mix of needy and avoidant behaviors. This "come here/get away" approach causes high anxiety and difficulty regulating emotions, resulting in low self-esteem and low trust in others.
Understanding Attachment Styles
Attachment styles are patterns of feeling, thinking, and behaving around emotions and conflict. They can change over time with effort and can vary with different caregivers. Recognizing your attachment style can help you understand your behaviors in relationships and work towards healthier connections.
I like this free Attachment Style assessment outside of an officially administrated test: https://www.attachmentproject.com/blog/four-attachment-styles/
*There are good critics that these initial assessments were not done with a broad enough sample size. There have been many follow up studies to work to validate the categories across cultures. However, I think it is still a working theory (as most things are) and worth holding in tension with diverse norms. People want to grab these studies and use them to dictate health/unhealthy and I think that can be tricky at best and dangerous at worst. I find this especially happens when religion or morals are superimposed onto them.