

attachment Fireworks: Why holiday Gatherings can Turn Into Anger You Didn't See Coming
Holiday anger often isn't about anger. It's panic and grief in disguise. A look at attachment, RAGE, and how to work through it when tempers flare.

Holidays carry memories of both togetherness and loss. Today's holiday, the Fourth of July, can bring up either side of that. Family visits, cookouts, long weekends with the same handful of people from morning to night. Or the absence of those gatherings: kids grown and gone, family members who've passed, living somewhere else now, a fallout that never got resolved. Either one can stir up old attachment wounds. Old roles come back. Old sore spots get touched. Someone brings up something from years ago, or nobody brings it up and the silence says just as much. And often what shows up first isn't sadness or fear. Alongside the fireworks outside, there's a different kind of combustion happening inside. It's anger.
It's easy to misread aggression. By design, it triggers fight, flight, or freeze in whoever is on the receiving end. Those are self-preserving modes, and in them it's nearly impossible to stay mindful or to do what Peter Fonagy calls mentalizing: accurately tracking what you think and feel, and what the other person thinks and feels, at the same time. Whether the anger is coming from someone else or from us, it's hard to tell in the moment whether the anger is really about anger, or whether it's covering something more vulnerable underneath.
This is especially true when anger is standing in for panic, and underneath that, grief.
The system underneath the anger
Attachment distress and attachment security are rooted in a brain system Jaak Panksepp called PANIC/GRIEF, working alongside two other systems called CARE and SEEKING. When disconnection happens and you need connection back, the automatic reaction is panic. That panic exists to alert you, and the people around you, that you need connection for survival. It teams up with SEEKING to point you toward the person you need. When that person notices your panic, it's their own CARE and SEEKING systems that pull them back toward you. These are old, fast circuits, and they run well beneath conscious thought.
When panic doesn't succeed in getting reconnection (through neglect or through attack) it risks tipping into the pain of isolation and grief. That's a state where you feel helpless, alone, and often like you don't matter. It can feel close enough to a threat to survival that the FEAR system recruits its counterpart, RAGE, to pull the system out of that collapse. RAGE brings a stronger, more mobilized feeling than panic or grief, and for a nervous system that's starting to feel it might not survive disconnection, that mobilization can feel like relief.
Why anger works, until it doesn't
Anger is empowering. Its original job, as Paul Ekman and Silvan Tomkins both described, is to clear whatever stands between you and something you're after. It comes with a sense of rightness and a jolt of confidence. Paired with SEEKING, it can help a person get real things done.
The problem is that in relationships, when anger is being called up in service of PANIC/GRIEF rather than in service of an actual obstacle, it tends to produce the opposite of what's needed. It pushes the other person away and adds to the misunderstanding instead of resolving it. The person on the receiving end usually focuses on the anger itself and misses the panic, grief, and fear driving it. That deepens the isolation, the helplessness, and the hit to self-worth that started the whole cycle.
From response to pattern
This pattern doesn't come from nowhere. It builds out of repeated experiences where attachment cues weren't met well, and over time the response becomes automatic. At the automatic, repeated level, we start calling it personality.
This particular pattern (anger that is really panic and grief in disguise) shows up more often in certain personality profiles: Borderline Personality Disorder, Narcissistic Personality Disorder, and in Enneagram terms, the one-to-one (sexual) subtypes of Eights, Ones, and Fours in particular. In each case, the anger looks like the presenting problem, but the attachment system underneath it is what actually needs attention.
What changes it
Change comes from three places: awareness, tools, and new experience.
Awareness means being able to mindfully notice when you're about to tip into this state, when you're in it, and what happened as a result once it's passed. That includes recognizing your own patterns: how you think, what you feel, where your eyes go, what happens in your body, how you move, and what you tend to say. A simple way to check yourself, or to notice it in someone else, is to ask what you tend to:
Think
Say
Feel
Do
Tools, from a Somatic Experiencing lens, give the nervous system a way to move through activation instead of getting stuck at the top of it or freezing under it.
Titration means taking the activation in small pieces instead of all at once. Rather than diving straight into the memory or the argument that set off the rage, you touch it briefly, notice what happens in the body, and back off before it overwhelms you. Small doses are easier for the nervous system to process and complete.
Pendulation is the rhythm of moving between that activation and a place of relative ease or resource, back and forth. You might notice the heat rising in your chest, then shift attention to your feet on the floor or a steady breath, then check back in with the heat. That back and forth is what teaches the body it can go into activation and come back out, instead of getting flooded.
Shifting attention in and out works alongside both. Attention in means noticing sensation, tension, temperature, and impulses to move. Attention out means noticing the room, another person's face, or something neutral and steady nearby. Moving between the two keeps you from getting swallowed by the internal experience or dissociating away from it entirely.
Tracking waves of activation and deactivation means watching the rise and fall as it happens rather than judging it. Rage has a shape: it builds, it peaks, and if you don't feed it or fight it, it comes back down. Learning to watch that curve, rather than either suppressing it or getting swept into it, is what turns rage from something that happens to you into something you can move through.
None of this is about stopping the anger before it starts. It's about staying present enough in your body to ride the wave instead of being ridden by it.
New experience comes from two places at once: growing confidence in your own capacity for self-regulation, and being met by people whose own nervous systems can stay regulated while yours isn't, people who can understand you and stay close to you through the storm instead of matching it or retreating from it.
Bringing it back to the holiday
If this weekend brings up a flash of irritation at a family member that threatens to turn into a blow up or painful drama, or you watch someone you love go from calm to furious over something small, try not to jump straight to conclusions about "bad behavior." Underneath a lot of holiday tempers is an old, fast circuit doing exactly what it was built to do: trying to get connection back before the isolation underneath becomes unbearable.
That doesn't excuse harm done in the heat of it. But it does point to where the real work is. Not in suppressing the anger and not in venting it, but in learning to recognize the panic and grief driving it, and building the capacity, in yourself and in your relationships, to stay close through the storm instead of being scattered by it.

Panic Attacks Aren't About Fear. They're About Being Left.
Most panic treatment targets fear. But panic and fear run on separate systems in the brain, with different chemistry, different circuitry, and different jobs. Understanding which one is actually firing changes what kind of help works.

Most people describe a panic attack the same way. It felt like dying. Like the room was closing in. Like something terrible was about to happen. So we treat panic like a fear problem. We teach breathing exercises, we challenge catastrophic thoughts, we tell the nervous system "you are safe right now," and sometimes that helps.
But it doesn't always help. I think that's because we're answering the wrong question. Panic isn't your brain asking "am I in danger?" It's an alert. An old, loud signal whose entire job is to maintain connection, by telling you, urgently, that you are disconnected right now or convinced that disconnection is about to happen.
Two different alarm systems
Your brain has more than one way to sound an alarm, and they're not the same circuit doing the same job at different volumes.
FEAR is the system that responds to a predator, a car swerving into your lane, a hand on a hot stove (by the way when something is all caps it means it’s a label for a brain system, when it’s not it means it is labeling an emotional feeling). It runs through the amygdala, it's fast, and it's built for immediate physical threat. This is the system most anxiety treatment is designed to address.
PANIC is different, and researchers actually call it PANIC/GRIEF, because it's one system with two faces. It runs a separate route from FEAR, through deep midbrain structures up to the anterior cingulate cortex, and it isn't regulated by the same threat chemistry. It runs largely on your body's own opioid system, the same chemistry involved in bonding and the comfort of closeness. When that opioid supply drops, the alarm goes off.
PANIC/GRIEF is unusual among the seven basic emotion systems in that its name captures two distinct phases of feeling. When panic does not result in feeling secure in connection or attachment again, or we have given up hope of that happening, our system collapses into the other side of that coin: an experience of grief. Grief is what it feels like when connection is already lost. It's the helplessness, the pain of isolation, the collapse that comes when there's nothing left to do about it. The feelings of panic come before that. PANIC's job isn't to cause us to brace for danger. It's to sound the alarm loudly enough, and urgently enough, that connection gets restored before it's lost for good. A panic attack is your system raising every biological and emotional signal it has, fast, because as far as it's concerned, the only thing standing between you and that collapse is whether the alarm works.
This is the same pattern researchers have long described in young mammals separated from a caregiver. First an active, distressed protest: calling out, searching, trying to restore contact. Only later, if reconnection doesn't come, a collapse into something quieter and more despairing. Panic is the protest call. It exists to bring someone back, or to bring you back to yourself, before the despair sets in.
This is also why a panic attack so often doesn't match the size of whatever triggered it. You're not overreacting to a small thing or having symptoms out of nowhere. A fast, old part of your brain has registered that the helplessness of isolation might be coming, and it's throwing everything it has at preventing that outcome, before you've even had time to name what's happening.
What "disconnection" actually means here
Surprisingly, the PANIC/GRIEF system doesn't only fire when someone physically leaves the room. It fires on a prediction (remember, the brain is a prediction machine, as neuropsychoanalyst Mark Solms has argued), and what it's predicting is whether GRIEF is about to arrive.
Underneath every panic attack is a fast, mostly unconscious assessment running on three things at once. A memory of what that helpless, isolated collapse has felt like before. A prediction about whether it's about to happen again right now. And a read on both yourself and the other person: whether you can survive being without them, whether they're still actually with you, whether this is the moment you finally fall into that state you already know.
That's why panic can show up in places that have nothing to do with relationships on the surface. A work presentation. A crowded store. A plane. What's actually being evaluated underneath isn't your presenting skills, the room, or the plane. It's closer to: "if this goes badly, will I end up alone with no way to fix it, and has that helplessness happened to me before?" If your history has taught your nervous system what that collapse feels like, your brain doesn't wait for it to arrive. It panics early, trying to head it off, because heading it off is the whole point of the system.
What's happening in your body
This system has a different chemical signature than fear does, and that's part of why fear-based treatment doesn't always land.
Where the FEAR system runs largely on CRF, norepinephrine, and the threat-detection chemistry of the amygdala, the PANIC/GRIEF system runs primarily on the brain's own opioids, along with oxytocin and prolactin, the same chemicals involved in bonding and the comfort of closeness. In animal studies, giving opioids is the single most effective way to quiet a separated infant's distress calls. That tells you what the alarm is actually built to respond to. Not threat reduction. Reconnection. It goes off when that opioid-driven sense of closeness drops, and it shuts off when closeness is restored, not when danger passes.
Here's the piece that explains what a panic attack actually feels like in the body. This circuit doesn't stop at producing an emotional signal. It directly regulates breathing, heart rate, and pain sensitivity as part of its basic function, and its territory overlaps with structures that also drive the body's fear and arousal chemistry, including norepinephrine. So when this alarm fires, it doesn't stay contained to "I feel disconnected." It recruits your sympathetic nervous system, the same system responsible for fight-or-flight, and that's where the racing heart, the shallow breathing, the sweating, and the trembling come from. The alert has to be loud enough, physically, to actually move you or someone else to act. A quiet signal doesn't restore connection. A racing heart and a flood of adrenaline-like chemistry does, because it's built to be impossible to ignore.
This is also why a panic attack can feel indistinguishable from a heart attack or a respiratory emergency. It isn't your imagination and it isn't "just anxiety." Your sympathetic nervous system has activated for real, your heart rate has climbed for real, your breathing has changed for real. The alarm is bodily because it has to be. A signal whose entire purpose is to summon connection back doesn't work if it's subtle.
The old proof: two problems, two drugs
Long before anyone had mapped this circuitry, clinicians stumbled onto evidence that panic and anxiety are actually two different problems, by accident, through a drug that only fixed one of them.
In 1960, a psychiatrist named Donald Klein was working at Hillside Hospital in Queens, New York, treating patients with severe anxiety attacks and agoraphobia. He was testing imipramine, one of the first antidepressants, which had only been introduced a few years earlier. What he found surprised him. Imipramine stopped the panic attacks themselves, often within weeks. But it didn't touch something else these patients were still carrying: the fear of having another attack. That anticipatory dread, and the avoidance behavior built around it, the not going to the store, the not getting on the plane, stuck around long after the attacks had stopped. It took a different kind of medication, an anti-anxiety drug, to work on that part.
Klein published this finding in 1962, and he called his method "pharmacological dissection." The logic was simple. If one drug stops the attacks and a different drug is needed for the fear of the attacks, you're probably not looking at one problem with two symptoms. You're looking at two different mechanisms that happen to sit next to each other. That observation eventually helped separate panic disorder from generalized anxiety disorder in psychiatric diagnosis, decades before anyone could point to the separate neurochemistry behind it.
It's a striking piece of history to sit next to everything above. Clinicians noticed, just from watching patients respond to medication, that panic and anxiety about panic were not the same thing and did not resolve through the same channel. That's the same split this whole piece has been describing, just discovered from the outside in, one prescription at a time, instead of from the inside out through brain circuitry.
Why this changes what helps
If panic is fundamentally a fear response, the treatment is exposure and reassurance. Prove to your nervous system that the room is not, in fact, dangerous.
If panic is fundamentally an attempt to maintain connection, the treatment has to focus on that. It's not enough to convince your nervous system that the plane won't crash, and it's not enough to slow the breathing once the sympathetic nervous system has already taken over, although that can help in the moment. The deeper work has two parts. One is with the prediction itself: what your body believes will happen, and what memory that belief is built on. The other is with your capacity to actually tolerate the thing panic is working so hard to avoid. As long as grief feels unsurvivable, the system has every reason to keep sounding the alarm rather than risk falling into it. Part of the work is building enough safety and support that helplessness and isolation, if they do show up, are no longer the catastrophe your body believes them to be.
This is part of why somatic and trauma informed approaches often reach panic in a way that pure cognitive reassurance doesn't. You can't think your way out of a prediction your body learned before you had words for it, and you can't think your way into trusting that grief, if it comes, is survivable. That trust tends to get built through relationship, through the body, through slowly proving to your nervous system, in small doses, that the helplessness it's so afraid of isn't the end of you.
The question underneath the question
If you've had a panic attack and wondered why "you're safe" never really helped, this might be why. Your nervous system wasn't asking about safety from harm. It was trying, urgently, to keep you from falling into a helplessness it’s known before.
That's not a flaw in your wiring. It's an old, well-intentioned system working as hard as it can to keep you from a pain it has every reason to believe is coming, sometimes in situations where that pain was never actually on the way. Understanding that doesn't make the panic disappear. But it changes what you're treating. You're not just talking your body out of a false alarm. You're slowly teaching it that even if grief came, you wouldn't be as alone in it as it fears.
An important note: most current clinical guidelines still treat panic attacks as an exaggerated fear response centered on the amygdala. The separation based view laid out here is a real, published alternative within affective neuroscience, but not something every researcher or clinician would sign off on. I find it more clinically useful for a lot of what shows up in the room, but it is a minority position within panic disorder research specifically, even though the PANIC/GRIEF system itself is well established as distinct from FEAR in the broader affective neuroscience literature.
References Used for this: The distinction between the FEAR and PANIC/GRIEF systems, including their separate neuroanatomy (amygdala and dorsal periaqueductal gray for FEAR; anterior cingulate, bed nucleus of the stria terminalis, and periaqueductal gray for PANIC/GRIEF) and their different core chemistry (CRF and norepinephrine for FEAR; endogenous opioids, oxytocin, and prolactin for PANIC/GRIEF), comes from the affective neuroscience research tradition built by Jaak Panksepp. It's summarized well in a 2020 paper by Gianni Francesetti, Antonio Alcaro, and Michele Settanni, "Panic disorder: attack of fear or acute attack of solitude? Convergences between affective neuroscience and phenomenological-Gestalt perspective," published in Research in Psychotherapy: Psychopathology, Process and Outcome. The protest and despair pattern in separated young mammals draws on John Bowlby's attachment research. The role of the PANIC/GRIEF circuit in directly regulating breathing, heart rate, and pain sensitivity, and the finding that opioids are the most effective known way to quiet separation distress calls in animal studies, are also drawn from that same research tradition. The sympathetic nervous system's role in producing panic attack symptoms such as rapid heart rate, shallow breathing, and sweating is well established in the clinical panic disorder literature more broadly. The imipramine finding comes from Klein DF, Fink M, "Psychiatric reaction patterns to imipramine," American Journal of Psychiatry, 1962;119:432-438, with later work on benzodiazepines and anticipatory anxiety summarized in Zitrin, Woerner, and Klein, 1981. Mark Solms's work on the brain as a predictive system draws on his 2021 book The Hidden Spring: A Journey to the Source of Consciousness.

Your Eyes Are Talking to Your Nervous System
Most people think about their eyes as the tools they use to see. What they don’t usually think about is that their eyes are part of their brain. Literally. In utero, the eyes separate from the same brain tissue that becomes everything else. The connection never goes away.

Most people think about their eyes as the tools they use to see. What they don’t usually think about is that their eyes are part of their brain. Literally. In utero, the eyes separate from the same brain tissue that becomes everything else. The connection never goes away.
My friend and colleague, Lillian Giocondo, turned me on to following the Biology of Trauma podcast, and a recent episode with neuro-optometrist Dr. Bryce Appelbaum grabbed my attention. Not because the information was fringe or surprising exactly, but because it put language to something we work with in Somatic Experiencing all the time.
In SE, we pay a lot of attention to the eyes.
We’ll sometimes ask a client to let their gaze soften. To notice what’s in their peripheral field without turning their head. To slowly move their eyes in different directions and notice what happens in the body. Or even to track our fingers and notice when the eye sight glitches. These aren’t quirky add-ons to the work. They’re rooted in the same biology Dr. Appelbaum describes.
Two-thirds of the neurons entering the brain come through the eyes. That’s not a small number. Your nervous system is constantly reading visual input to decide whether you’re safe or in danger. And one of the clearest signals it looks for is whether your peripheral vision is open.
When the nervous system shifts into fight or flight, peripheral vision collapses. The world narrows. You stop seeing what’s beside you and start locking onto what’s in front of you. This is your threat response working exactly as designed. The problem is that for many people who carry stored trauma or chronic stress, that narrowing becomes the default. The tunnel becomes baseline.
Dr. Appelbaum describes this as the body adapting to a tunneled state. The brain stops expecting wide vision. It reorganizes. And over time, people describe feeling like they’re looking through paper towel rolls. Which is just their eyes staying in a survival state.
In SE, one type of eye work we do is called, “orienting.” When a client can slowly, voluntarily move their eyes around the room and allow their eyes stop and focus on what they see, that’s the nervous system checking in with reality and finding it safe. The body follows. Shoulders often drop. Breath often comes in a little more easily.
Dr. Appelbaum introduces three simple exercises in the episode: peripheral pointing, eye push-ups, and eye stretches. Peripheral pointing involves fixing your gaze on a point in the room and then noticing, without moving your eyes, what else is out there. Pointing to it. Then checking. It rebuilds the body’s sense of being in space rather than locked into a single threat point.
These exercises build the same capacity we’re reaching for in SE. The ability to be in a body that can take in more of the world, to have more capacity not just tolerance. A nervous system that isn’t white-knuckling.
If you’ve ever wondered why we slow things down in trauma therapy, why we ask what you notice in your body or what catches your eye in the room, or to stop and feel into your eyes, this episode offers one clear answer. The eyes are not passive recorders. They’re active participants in whether you feel okay right now.
Is This Trauma or Just Stress? How to Tell the Difference.
Struggling to tell if it’s trauma or just stress? Learn a simple way to understand your reactions and how trauma therapy in Kansas City can help you heal.

Many people in Kansas City come to therapy unsure whether what they’re feeling is stress, burnout, or trauma. With trauma being talked about on podcasts and social media, it can feel like everything counts as trauma now. Commentators like Scott Galloway even argue that therapy tries to “explain everything with trauma” on The Prof G Podcast (Galloway, 2025).
There’s a real point here: when clinical words leave the therapy room, they often get stretched and lose their meaning. Trauma is one of those words.
A Simple Way to Compare Stress and Trauma
Here’s a helpful way to picture the difference. Think of reactions like money:
A $10 reaction to a $10 problem → normal stress
A $10 reaction to a $1 problem → a bad day
A $100 reaction to a $10 problem → old experiences may be involved
A $100 reaction to a $1 problem → often trauma residue
Not all distress is trauma, and not all trauma looks like the size of the situation you’re in.
So What Actually Counts as Trauma?
Clinically, trauma is not defined by the event.
It’s defined by what happens after the event.
Somatic researcher Peter Levine describes trauma as what happens when the nervous system can’t complete its stress response and return to normal (Levine, 1997; 2010).
In plain language:
Trauma is not what happened. Trauma is what stayed in the body afterward.
Two people can go through the same experience and have different outcomes:
one returns to baseline → stress
one stays stuck → trauma
This difference is about physiology and survival, not personal weakness.
Stress Is About Now. Trauma Is About Then.
A simple way to tell the difference:
Stress
has a clear cause
matches the size of the problem
fades when life calms down
Trauma patterns
show up in different situations
feel too big for the moment
don’t automatically go away even when life improves
Stress is your nervous system responding to today.
Trauma is your nervous system responding to back then.
How Trauma Shows Up (Even If You Don’t Call It Trauma)
Unfinished stress responses can look like:
shutting down during conflict
panic around feedback
feeling “on alert” in relationships
expecting the worst in small situations
people-pleasing to feel safe
Affective neuroscience shows these reactions begin in deeper emotional circuits (Panksepp, 1998; Solms, 2021), which is why you can’t simply “think your way out” of them.
Trauma Therapy in Kansas City
If you’re asking “Is this trauma or just stress?” a more useful question might be:
Am I spending today’s money — or yesterday’s?
At Analog Counseling in Overland Park, we help clients from across Kansas City complete unfinished stress responses and return to regulation. We use trauma-informed approaches including Somatic Experiencing, psychodynamic therapy, and neurobiological models.
We see clients from:
Overland Park
Kansas City, MO
Leawood
Olathe
Prairie Village
Lenexa
North Kansas City, MO
Lawrence
Gardner
And more!
A Note on Worthiness
You don’t have to wait for things to “get bad enough.”
Trauma therapy is about helping your nervous system settle and feel safe again — not proving that something happened.
References
American Psychiatric Association. (2022). DSM-5-TR.
Galloway, S. (2025). The Prof G Podcast.
Levine, P. (1997). Waking the Tiger.
Levine, P. (2010). In an Unspoken Voice.
Panksepp, J. (1998). Affective Neuroscience.
Schore, A. (2012). The Science of the Art of Psychotherapy.
Solms, M. (2021). The Hidden Spring.
van der Kolk, B. (2014). The Body Keeps the Score.
Understanding Inner Attention: A Path to Emotional Awareness
Have you ever noticed how you're constantly aware of your inner experiences - feeling anxious before a presentation, or bored during a long meeting? This natural awareness is what we call "attention inward." While we all do this automatically throughout our day, there's a deeper, more intentional way of turning our attention inward that's used in therapeutic approaches like Somatic Experiencing. This specialized practice can reveal insights about ourselves that usually remain hidden.

In a previous post we talked about attention out. In this post we’ll talk about attention in.
Have you ever noticed how you're constantly aware of your inner experiences - feeling anxious before a presentation, or bored during a long meeting? This natural awareness is what we call "attention inward." While we all do this automatically throughout our day, there's a deeper, more intentional way of turning our attention inward that's used in therapeutic approaches like Somatic Experiencing. This specialized practice can reveal insights about ourselves that usually remain hidden.
How Emotions Guide Us
Dr. Mark Solms's research helps us understand that emotions aren't just feelings - they're sophisticated guidance systems that help us survive and thrive. Think of emotions as messengers carrying important information. When we feel sad, for instance, that sadness is telling us we've lost something meaningful. More importantly, it's guiding us toward natural ways to heal: crying, seeking comfort from loved ones, or taking time for self-care.
But what happens when we can't follow these natural emotional pathways? Maybe we grew up learning that "big kids don't cry" or that showing vulnerability is weakness. When this happens, we develop coping mechanisms - like pushing the feeling away, distracting ourselves, or rationalizing why we shouldn't feel that way. Over time, these coping strategies become so automatic that we mistake them for our natural responses. It's like creating a detour around a blocked road and eventually forgetting the original route altogether.
A Different Way of Paying Attention
This is where intentional inner attention becomes valuable. By carefully observing our internal experience, we can reconnect with our authentic emotional responses that have been masked by years of coping strategies. Somatic Experiencing offers a helpful framework for this kind of attention through the SIBAM model:
Sensations: Physical feelings in your body (butterflies in your stomach, chest tightness, warmth, tingling)
Images: Mental pictures or memories that arise
Behaviors: Natural impulses to move or react
Affect: Conscious emotional experiences
Meaning: Our thoughts and interpretations
In our thinking-focused culture, we often jump straight to meaning-making - trying to analyze and understand before we've fully experienced our emotions. However, if we can learn to pause and first notice our bodily sensations, images, and impulses, we often discover clearer and more authentic information about our emotional needs.
This patient, body-first approach helps us bypass our habitual coping mechanisms and reconnect with our natural emotional wisdom. By learning to pay attention in this way, we can begin to untangle the difference between our authentic responses and our learned coping strategies.
Understanding Your Body's Alert System: A Guide to Feeling Safer in Everyday Life
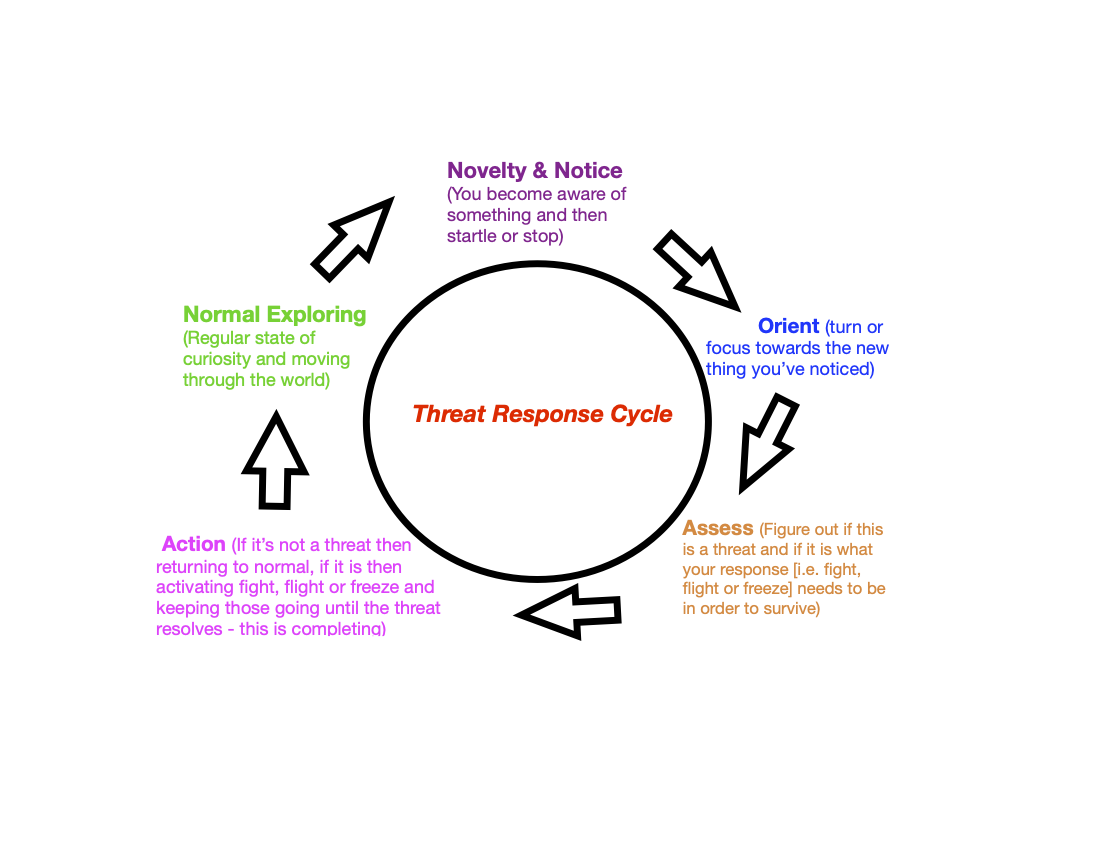
Ever notice how your body reacts when you open a stressful email or get into an argument? That racing heart, those tense shoulders - these aren't random reactions. They're part of your body's natural alert system called the threat response cycle, and understanding this system can change your life in wonderful ways.
Ever notice how your body reacts when you open a stressful email or get into an argument? That racing heart, those tense shoulders - these aren't random reactions. They're part of your body's natural alert system called the threat response cycle, and understanding this system can change your life in wonderful ways.
Your Built-In Safety System
Think of your body as having a special safety alarm, an instinct for safety. Just like our ancestors needed this alarm to stay safe from wild animals, we use it today in our modern world. This system kicks in when:
Reading a difficult email
Sitting through a tense meeting
Having a disagreement with someone you love
Walking into a crowded restaurant
Even chatting with a friend when a sensitive topic comes up
The Threat Response Cycle
Why Understanding This Matters
When you know how your alert system works, you gain a superpower: the ability to pause and check if you really need to be on high alert. Sometimes your alarm might go off when you're actually safe, like feeling panicked about giving a presentation to friendly colleagues. Other times, you might not notice real warning signs when you should, like staying in an unhealthy situation for too long.
Taking Back Control
The good news? Once you recognize when your alert system is active, you can:
Take a moment to pause
Look around and check if there's a real reason for concern
Choose how to respond rather than just react
Return to feeling calm and present when you realize you're safe
This awareness helps you move through your day with more peace and confidence. Instead of being controlled by automatic reactions, you can choose how to respond to life's challenges.
Remember: Your alert system isn't your enemy - it's trying to protect you! Learning to work with it, rather than against it, can help you feel more in control and at peace in your daily life.
Finding Peace Through 'Attention Out': A Simple First Step to Feeling Better
When you're feeling overwhelmed or stressed, your first instinct might be to dive deep into your thoughts and feelings. While this is completely natural, there's actually a gentler way to begin your healing journey. It's called "attention out," and it's simpler than you might think.

In another post we talk about attention In. In this post we’ll talk about attention out.
When you're feeling overwhelmed or stressed, your first instinct might be to dive deep into your thoughts and feelings. While this is completely natural, there's actually a gentler way to begin your healing journey. It's called "attention out," and it's simpler than you might think.
What is "Attention Out"?
Think of your attention like a flashlight. You can shine it inward (on your thoughts, feelings, and body sensations) or outward (on the world around you). Both are important, but learning to focus outward first can help you feel more grounded and safe.
Why Start with Looking Outward?
When you first come to counseling, you might want to jump right in and talk about everything that's troubling you. That's completely normal! But starting with "attention out" first is like giving your mind a gentle reset button. It helps your body recognize that right now, in this moment, you're safe.
How to Practice "Attention Out": A Simple Exercise
Here's a simple practice called "orienting" that you can try right now. Orienting is a part of a larger instinct for safety called, the threat response cycle.
Find a comfortable spot to sit
Let your eyes wander naturally around your surroundings
Notice what catches your attention - maybe it's a color, a shape, or an object
Don't worry about why something catches your eye - just let your gaze move freely
Try to set aside your thoughts for a moment and just focus on what you see
What You Might Experience
When you practice this, you might notice some natural changes:
Your breathing might become deeper
Colors might seem brighter
Your body might feel more relaxed
You might feel more present in the moment
These are all signs that your body is finding its natural balance.
Why This Works
Your body has a natural ability to heal and find balance. Sometimes it just needs a little help remembering how. "Attention out" is like giving your nervous system a gentle reminder that it can relax and reset (Levine, 1997; 2010).
Remember: This might feel strange at first, and that's okay! Like any new skill, it takes practice. The key is to be patient with yourself as you learn this new way of finding calm.
Beyond Talk Therapy: Discovering Somatic Experiencing
There's a special way to help with feelings that are hard to access or even know about. It's called Somatic Experiencing.

Why We Think and Talk
We think and talk for lots of reasons. One of those reasons is to feel better. Let's explore this more.
How Thinking and Talking Help Us
When we feel something strong inside, we want to let it out. This brings us relief and contributes to our life. Here are some examples:
- When we're sad, talking to someone helps us feel less sad and understand ourselves better
- When we're angry, we might want to rant to someone about what's bothering us, think about how to solve what’s bothering us and maybe even fantasize about what we could have done differently, all in an attempt to feel less angry.
- When we do something good, we want to share it with others, this helps us feel more whole and happy.
- When we’re intrigued about something we think about what’s grabbed our attention in order to enjoy the exploration and hopefully to eventually feel the relief of understanding
Our feelings are like messages from our body. They tell us what is going on and what we need to feel better and live happier lives.
Why Some Feelings Are Hard to Notice or Talk About
Sometimes when we share our feelings, things don't go well. Maybe someone didn't listen, or we got hurt. When this happens, we might start automatically hiding these feelings, even from ourselves and even before we know we’re having them. This can make us feel worse over time. They can even cause us to misunderstand the present, to confuse our current situation with the past and react poorly because of that. With feelings that are stuck, out of our awareness and causing us problems talking and thinking alone are about the slowest ways there are to feel better. And often then only keep us stuck.
A Different Way to Feel Better
There's a special way to help with feelings that are hard to access or even know about. It's called Somatic Experiencing. Instead of just talking, we:
- Pay attention to your body and the sensations inside
- Allow some of the movements from spontaneous impulses in the body
- Learn how to navigate activation and de-activation in the body which helps you deal with stuck, pent up feelings little by little instead of in an overwhelming way.
- Empowers you
- Plus much more
Someone trained in Somatic Experiencing helps you do this safely. They teach you how to listen to your body and understand what it's telling you. While you still talk about your feelings, you also learn to feel them in a way that's comfortable and safe. This brings things that are unconscious to the light of day and lets them out so you feel better and live easier.
All of which helps you find answers that come from deep inside yourself, making you feel more sure about what you need.
A great article in the nyt on somatic experiencing!
This article explores the concept of somatic therapy, which focuses on healing emotional wounds through the body.

Illustration by Daniel Barreto
New York Times Article on Somatic Experiencing Link
The article explores the concept of somatic therapy, which focuses on healing emotional wounds through the body. The author describes their personal experience with a therapist who uses somatic techniques to address their anxiety and fear of failure. The article delves into the principles of somatic experiencing (S.E.), a type of therapy that emphasizes the body's role in emotional processing. The author discusses the benefits of S.E., such as reducing anxiety, improving emotional regulation, and promoting overall well-being. The article also highlights the growing popularity of somatic therapy and the increasing demand for practitioners.
Curious? Book a Somatic Experiencing session with Aaron today.