

Why Panic Can Feel Like It Comes From Nowhere
A companion piece to "Panic Attacks Aren't About Fear." Why panic so often hits without warning, and what the divided brain has to do with it.

One of the strangest things about panic is how often it arrives without a story attached. There's no clear reason, nothing you can point to, just the alarm going off in the middle of an ordinary moment.
In an earlier piece, I wrote about panic as an attachment alarm rather than a fear response. Panic isn't your brain asking "am I in danger?" It's an old, loud signal built to maintain connection, telling you that you're disconnected right now, or convinced that disconnection is about to happen. That system, which researchers call PANIC/GRIEF, runs on different chemistry than fear does and directly affects your breathing, heart rate, and pain sensitivity, which is why the alarm shows up as a full-body event rather than just a thought.
What I want to get into here is a different question. Why does the alarm so often go off with no obvious trigger? Why does it feel like it's coming from nowhere?
Two kinds of attention
I think part of the answer has to do with how the two halves of the brain handle information differently, an idea the psychiatrist Iain McGilchrist has spent much of his career working out.
His argument isn't the old, oversimplified version you may have heard, that the left brain does logic and the right brain does creativity. McGilchrist's case is that the two hemispheres aren't divided by subject matter at all. They're divided by the kind of attention each one pays to the world. Both hemispheres are involved in most of what the brain does. They just interact with experience in different ways.
The right hemisphere takes in the whole picture at once: context, relationship, body state, the things that are true but haven't been put into words yet. It's comfortable holding something ambiguous without rushing to resolve it. The left hemisphere works differently. It wants the explicit, the categorized, the already-known. It's fast and confident, and according to McGilchrist, it doesn't know what it doesn't know. If something doesn't fit a category it already has, the left hemisphere tends to filter it out rather than sit with the uncertainty.
McGilchrist also argues that the right hemisphere is more closely tied to the body, to reading relational and emotional cues, and to intense emotional states in general, especially the harder ones like fear and distress.
A signal with nowhere to go
Put those two pieces together and it starts to make sense how you can know something and not know it at the same time.
It's entirely possible for your right hemisphere to pick up on something real: a shift in someone's tone, a withdrawal, a relationship that's fraying, a sense that you're more alone in a room full of people than you should be. All of that can register well before it can be put into words or sorted into a category the left hemisphere will accept. If the left hemisphere can't find a clean, explicit story for what's being sensed, it may not integrate the signal at all. The information doesn't vanish. It just doesn't make it into the version of events you're consciously telling yourself.
So the body notices something and signals it, but the signal has no way into the ordinary channel of thought and language. This might be part of why Freud paid such close attention to slips of the tongue, words that come out unintended and seem out of place, and to dream interpretation, even though he wouldn't have described it in these terms. Both were attempts to reach content that was present but blocked from conscious, verbal access. The PANIC/GRIEF system doesn't need permission from your conscious narrative to act. If the felt sense of disconnection is strong enough and the explicit story isn't catching up to it, the alarm keeps escalating until it's loud enough that you can't ignore it. That's one way to understand why panic so often hits with no obvious trigger. The trigger was there. It just didn't pass through the part of the brain that explains things to you in words.
Why this matters for treatment
This is a contested area of neuroscience. McGilchrist's broader claims about the hemispheres have real critics, and some argue he overstates how cleanly these functions divide. So know that this isn't settled fact.
But the narrower point, that something can be accurately sensed in the body and in relationship before it's consciously articulated, fits well with what's already known about how the PANIC/GRIEF system works. It doesn't wait for you to have a sentence ready. It acts on what's felt, not on what's been said yet.
That has a practical implication. If the original signal never passed through the part of you built to name, define, and explain things in words, then reassuring yourself in that same verbal mode is less likely to help than something that can reach the signal where it actually lives. You can tell someone, accurately, that there's no danger in the room, and it can still miss the point, because the alarm was never about the room. This is a big part of why somatic and body-based approaches tend to reach panic in a way that talking alone doesn't. The work isn't just building a better explanation. It's helping the part of you that senses things before it can name them learn, slowly, that it's not as alone as it fears, and that it now has more capacity to handle grief and aloneness than it did back when it first learned to be afraid of them.
Reference notes: McGilchrist's claims about hemispheric attention styles, the right hemisphere's role in holding ambiguity and context, the left hemisphere's tendency toward premature categorization and closure, and the right hemisphere's closer relationship to bodily and relational awareness, come from his 2009 book The Master and His Emissary: The Divided Brain and the Making of the Western World and his 2021 follow-up The Matter with Things. These claims are influential but not uncontested. Michael Spezio, a psychologist at Scripps College, published a critical assessment in 2019, "McGilchrist and hemisphere lateralization: a neuroscientific and metaanalytic assessment," in the journal Religion, Brain & Behavior, arguing that recent meta-analyses do not support the sweeping, oppositional picture of hemispheric difference McGilchrist describes. The connection between this framework and panic attacks specifically is my own synthesis, drawn from putting McGilchrist's model of attention alongside the PANIC/GRIEF research of Jaak Panksepp covered in the companion piece, not a claim McGilchrist has made himself.

Panic Attacks Aren't About Fear. They're About Being Left.
Most panic treatment targets fear. But panic and fear run on separate systems in the brain, with different chemistry, different circuitry, and different jobs. Understanding which one is actually firing changes what kind of help works.

Most people describe a panic attack the same way. It felt like dying. Like the room was closing in. Like something terrible was about to happen. So we treat panic like a fear problem. We teach breathing exercises, we challenge catastrophic thoughts, we tell the nervous system "you are safe right now," and sometimes that helps.
But it doesn't always help. I think that's because we're answering the wrong question. Panic isn't your brain asking "am I in danger?" It's an alert. An old, loud signal whose entire job is to maintain connection, by telling you, urgently, that you are disconnected right now or convinced that disconnection is about to happen.
Two different alarm systems
Your brain has more than one way to sound an alarm, and they're not the same circuit doing the same job at different volumes.
FEAR is the system that responds to a predator, a car swerving into your lane, a hand on a hot stove (by the way when something is all caps it means it’s a label for a brain system, when it’s not it means it is labeling an emotional feeling). It runs through the amygdala, it's fast, and it's built for immediate physical threat. This is the system most anxiety treatment is designed to address.
PANIC is different, and researchers actually call it PANIC/GRIEF, because it's one system with two faces. It runs a separate route from FEAR, through deep midbrain structures up to the anterior cingulate cortex, and it isn't regulated by the same threat chemistry. It runs largely on your body's own opioid system, the same chemistry involved in bonding and the comfort of closeness. When that opioid supply drops, the alarm goes off.
PANIC/GRIEF is unusual among the seven basic emotion systems in that its name captures two distinct phases of feeling. When panic does not result in feeling secure in connection or attachment again, or we have given up hope of that happening, our system collapses into the other side of that coin: an experience of grief. Grief is what it feels like when connection is already lost. It's the helplessness, the pain of isolation, the collapse that comes when there's nothing left to do about it. The feelings of panic come before that. PANIC's job isn't to cause us to brace for danger. It's to sound the alarm loudly enough, and urgently enough, that connection gets restored before it's lost for good. A panic attack is your system raising every biological and emotional signal it has, fast, because as far as it's concerned, the only thing standing between you and that collapse is whether the alarm works.
This is the same pattern researchers have long described in young mammals separated from a caregiver. First an active, distressed protest: calling out, searching, trying to restore contact. Only later, if reconnection doesn't come, a collapse into something quieter and more despairing. Panic is the protest call. It exists to bring someone back, or to bring you back to yourself, before the despair sets in.
This is also why a panic attack so often doesn't match the size of whatever triggered it. You're not overreacting to a small thing or having symptoms out of nowhere. A fast, old part of your brain has registered that the helplessness of isolation might be coming, and it's throwing everything it has at preventing that outcome, before you've even had time to name what's happening.
What "disconnection" actually means here
Surprisingly, the PANIC/GRIEF system doesn't only fire when someone physically leaves the room. It fires on a prediction (remember, the brain is a prediction machine, as neuropsychoanalyst Mark Solms has argued), and what it's predicting is whether GRIEF is about to arrive.
Underneath every panic attack is a fast, mostly unconscious assessment running on three things at once. A memory of what that helpless, isolated collapse has felt like before. A prediction about whether it's about to happen again right now. And a read on both yourself and the other person: whether you can survive being without them, whether they're still actually with you, whether this is the moment you finally fall into that state you already know.
That's why panic can show up in places that have nothing to do with relationships on the surface. A work presentation. A crowded store. A plane. What's actually being evaluated underneath isn't your presenting skills, the room, or the plane. It's closer to: "if this goes badly, will I end up alone with no way to fix it, and has that helplessness happened to me before?" If your history has taught your nervous system what that collapse feels like, your brain doesn't wait for it to arrive. It panics early, trying to head it off, because heading it off is the whole point of the system.
What's happening in your body
This system has a different chemical signature than fear does, and that's part of why fear-based treatment doesn't always land.
Where the FEAR system runs largely on CRF, norepinephrine, and the threat-detection chemistry of the amygdala, the PANIC/GRIEF system runs primarily on the brain's own opioids, along with oxytocin and prolactin, the same chemicals involved in bonding and the comfort of closeness. In animal studies, giving opioids is the single most effective way to quiet a separated infant's distress calls. That tells you what the alarm is actually built to respond to. Not threat reduction. Reconnection. It goes off when that opioid-driven sense of closeness drops, and it shuts off when closeness is restored, not when danger passes.
Here's the piece that explains what a panic attack actually feels like in the body. This circuit doesn't stop at producing an emotional signal. It directly regulates breathing, heart rate, and pain sensitivity as part of its basic function, and its territory overlaps with structures that also drive the body's fear and arousal chemistry, including norepinephrine. So when this alarm fires, it doesn't stay contained to "I feel disconnected." It recruits your sympathetic nervous system, the same system responsible for fight-or-flight, and that's where the racing heart, the shallow breathing, the sweating, and the trembling come from. The alert has to be loud enough, physically, to actually move you or someone else to act. A quiet signal doesn't restore connection. A racing heart and a flood of adrenaline-like chemistry does, because it's built to be impossible to ignore.
This is also why a panic attack can feel indistinguishable from a heart attack or a respiratory emergency. It isn't your imagination and it isn't "just anxiety." Your sympathetic nervous system has activated for real, your heart rate has climbed for real, your breathing has changed for real. The alarm is bodily because it has to be. A signal whose entire purpose is to summon connection back doesn't work if it's subtle.
The old proof: two problems, two drugs
Long before anyone had mapped this circuitry, clinicians stumbled onto evidence that panic and anxiety are actually two different problems, by accident, through a drug that only fixed one of them.
In 1960, a psychiatrist named Donald Klein was working at Hillside Hospital in Queens, New York, treating patients with severe anxiety attacks and agoraphobia. He was testing imipramine, one of the first antidepressants, which had only been introduced a few years earlier. What he found surprised him. Imipramine stopped the panic attacks themselves, often within weeks. But it didn't touch something else these patients were still carrying: the fear of having another attack. That anticipatory dread, and the avoidance behavior built around it, the not going to the store, the not getting on the plane, stuck around long after the attacks had stopped. It took a different kind of medication, an anti-anxiety drug, to work on that part.
Klein published this finding in 1962, and he called his method "pharmacological dissection." The logic was simple. If one drug stops the attacks and a different drug is needed for the fear of the attacks, you're probably not looking at one problem with two symptoms. You're looking at two different mechanisms that happen to sit next to each other. That observation eventually helped separate panic disorder from generalized anxiety disorder in psychiatric diagnosis, decades before anyone could point to the separate neurochemistry behind it.
It's a striking piece of history to sit next to everything above. Clinicians noticed, just from watching patients respond to medication, that panic and anxiety about panic were not the same thing and did not resolve through the same channel. That's the same split this whole piece has been describing, just discovered from the outside in, one prescription at a time, instead of from the inside out through brain circuitry.
Why this changes what helps
If panic is fundamentally a fear response, the treatment is exposure and reassurance. Prove to your nervous system that the room is not, in fact, dangerous.
If panic is fundamentally an attempt to maintain connection, the treatment has to focus on that. It's not enough to convince your nervous system that the plane won't crash, and it's not enough to slow the breathing once the sympathetic nervous system has already taken over, although that can help in the moment. The deeper work has two parts. One is with the prediction itself: what your body believes will happen, and what memory that belief is built on. The other is with your capacity to actually tolerate the thing panic is working so hard to avoid. As long as grief feels unsurvivable, the system has every reason to keep sounding the alarm rather than risk falling into it. Part of the work is building enough safety and support that helplessness and isolation, if they do show up, are no longer the catastrophe your body believes them to be.
This is part of why somatic and trauma informed approaches often reach panic in a way that pure cognitive reassurance doesn't. You can't think your way out of a prediction your body learned before you had words for it, and you can't think your way into trusting that grief, if it comes, is survivable. That trust tends to get built through relationship, through the body, through slowly proving to your nervous system, in small doses, that the helplessness it's so afraid of isn't the end of you.
The question underneath the question
If you've had a panic attack and wondered why "you're safe" never really helped, this might be why. Your nervous system wasn't asking about safety from harm. It was trying, urgently, to keep you from falling into a helplessness it’s known before.
That's not a flaw in your wiring. It's an old, well-intentioned system working as hard as it can to keep you from a pain it has every reason to believe is coming, sometimes in situations where that pain was never actually on the way. Understanding that doesn't make the panic disappear. But it changes what you're treating. You're not just talking your body out of a false alarm. You're slowly teaching it that even if grief came, you wouldn't be as alone in it as it fears.
An important note: most current clinical guidelines still treat panic attacks as an exaggerated fear response centered on the amygdala. The separation based view laid out here is a real, published alternative within affective neuroscience, but not something every researcher or clinician would sign off on. I find it more clinically useful for a lot of what shows up in the room, but it is a minority position within panic disorder research specifically, even though the PANIC/GRIEF system itself is well established as distinct from FEAR in the broader affective neuroscience literature.
References Used for this: The distinction between the FEAR and PANIC/GRIEF systems, including their separate neuroanatomy (amygdala and dorsal periaqueductal gray for FEAR; anterior cingulate, bed nucleus of the stria terminalis, and periaqueductal gray for PANIC/GRIEF) and their different core chemistry (CRF and norepinephrine for FEAR; endogenous opioids, oxytocin, and prolactin for PANIC/GRIEF), comes from the affective neuroscience research tradition built by Jaak Panksepp. It's summarized well in a 2020 paper by Gianni Francesetti, Antonio Alcaro, and Michele Settanni, "Panic disorder: attack of fear or acute attack of solitude? Convergences between affective neuroscience and phenomenological-Gestalt perspective," published in Research in Psychotherapy: Psychopathology, Process and Outcome. The protest and despair pattern in separated young mammals draws on John Bowlby's attachment research. The role of the PANIC/GRIEF circuit in directly regulating breathing, heart rate, and pain sensitivity, and the finding that opioids are the most effective known way to quiet separation distress calls in animal studies, are also drawn from that same research tradition. The sympathetic nervous system's role in producing panic attack symptoms such as rapid heart rate, shallow breathing, and sweating is well established in the clinical panic disorder literature more broadly. The imipramine finding comes from Klein DF, Fink M, "Psychiatric reaction patterns to imipramine," American Journal of Psychiatry, 1962;119:432-438, with later work on benzodiazepines and anticipatory anxiety summarized in Zitrin, Woerner, and Klein, 1981. Mark Solms's work on the brain as a predictive system draws on his 2021 book The Hidden Spring: A Journey to the Source of Consciousness.

Your Eyes Are Talking to Your Nervous System
Most people think about their eyes as the tools they use to see. What they don’t usually think about is that their eyes are part of their brain. Literally. In utero, the eyes separate from the same brain tissue that becomes everything else. The connection never goes away.

Most people think about their eyes as the tools they use to see. What they don’t usually think about is that their eyes are part of their brain. Literally. In utero, the eyes separate from the same brain tissue that becomes everything else. The connection never goes away.
My friend and colleague, Lillian Giocondo, turned me on to following the Biology of Trauma podcast, and a recent episode with neuro-optometrist Dr. Bryce Appelbaum grabbed my attention. Not because the information was fringe or surprising exactly, but because it put language to something we work with in Somatic Experiencing all the time.
In SE, we pay a lot of attention to the eyes.
We’ll sometimes ask a client to let their gaze soften. To notice what’s in their peripheral field without turning their head. To slowly move their eyes in different directions and notice what happens in the body. Or even to track our fingers and notice when the eye sight glitches. These aren’t quirky add-ons to the work. They’re rooted in the same biology Dr. Appelbaum describes.
Two-thirds of the neurons entering the brain come through the eyes. That’s not a small number. Your nervous system is constantly reading visual input to decide whether you’re safe or in danger. And one of the clearest signals it looks for is whether your peripheral vision is open.
When the nervous system shifts into fight or flight, peripheral vision collapses. The world narrows. You stop seeing what’s beside you and start locking onto what’s in front of you. This is your threat response working exactly as designed. The problem is that for many people who carry stored trauma or chronic stress, that narrowing becomes the default. The tunnel becomes baseline.
Dr. Appelbaum describes this as the body adapting to a tunneled state. The brain stops expecting wide vision. It reorganizes. And over time, people describe feeling like they’re looking through paper towel rolls. Which is just their eyes staying in a survival state.
In SE, one type of eye work we do is called, “orienting.” When a client can slowly, voluntarily move their eyes around the room and allow their eyes stop and focus on what they see, that’s the nervous system checking in with reality and finding it safe. The body follows. Shoulders often drop. Breath often comes in a little more easily.
Dr. Appelbaum introduces three simple exercises in the episode: peripheral pointing, eye push-ups, and eye stretches. Peripheral pointing involves fixing your gaze on a point in the room and then noticing, without moving your eyes, what else is out there. Pointing to it. Then checking. It rebuilds the body’s sense of being in space rather than locked into a single threat point.
These exercises build the same capacity we’re reaching for in SE. The ability to be in a body that can take in more of the world, to have more capacity not just tolerance. A nervous system that isn’t white-knuckling.
If you’ve ever wondered why we slow things down in trauma therapy, why we ask what you notice in your body or what catches your eye in the room, or to stop and feel into your eyes, this episode offers one clear answer. The eyes are not passive recorders. They’re active participants in whether you feel okay right now.
Trauma Isn’t Intensity — It’s What the Nervous System Learns
When people hear the word trauma, they often picture something overwhelming: extreme fear, intense emotion, or a catastrophic event. And while trauma can involve intense experiences, defining it primarily by emotional intensity actually misses the heart of the matter. Trauma is not best understood as how big something felt — but as what the nervous system learned when survival was at stake.

When people hear the word trauma, they often picture something overwhelming: extreme fear, intense emotion, or a catastrophic event. And while trauma can involve intense experiences, defining it primarily by emotional intensity actually misses the heart of the matter. Trauma is not best understood as how big something felt — but as what the nervous system learned when survival was at stake.
From a nervous-system perspective, trauma begins with threat. When we perceive danger, the body mobilizes automatically to protect us through fight, flight, or freeze. This mobilization requires a rapid surge of energy — heart rate increases, muscles tense, attention narrows. This temporary dysregulation is not a problem; it is the body doing exactly what it is designed to do.
Under normal circumstances, that survival energy is spent. We run, resist, escape, or orient toward safety. Once the threat passes and the energy is discharged, the nervous system returns to its baseline rhythm of regulation and flexibility.
Trauma occurs when that process is interrupted.
When a threat cannot be escaped, fought, or fully responded to — because of powerlessness, overwhelm, developmental immaturity, or relational constraints — the nervous system is forced to cope rather than complete the survival cycle. The energy meant for action remains trapped in the body. This unresolved dysregulation is profoundly uncomfortable, and the system adapts in whatever way it can to endure.
Over time, this unfinished survival response becomes encoded as learning.
As Mark Solms explains in The Feeling Brain, affect is fundamentally tied to homeostasis — the body’s drive to regulate internal states. Trauma represents a disruption in this regulatory process. The system does not simply remember what happened; it remembers how it survived.
Similarly, Stephen Porges shows through Polyvagal Theory that our nervous systems continuously assess safety and danger beneath conscious awareness. When safety cannot be restored, the system defaults to defensive strategies — hyperarousal, collapse, shutdown — not as pathology, but as protection.
Crucially, the coping strategies used during the original threat often replace instinctive responses in the future. Instead of fluid fight or flight, the body replays learned patterns. This is why trauma can show up in two seemingly opposite ways: explosive emotional reactions that feel disproportionate to the present moment, or a puzzling absence of response when action would be appropriate. In both cases, the nervous system is responding to past threat in the present.
As Allan Schore emphasizes, trauma is ultimately a disorder of affect regulation. It is not the event itself that defines trauma, but whether the nervous system could return to regulated flow afterward — especially in the presence of attuned support.
Understanding trauma this way reframes healing. The work is not primarily about revisiting intense emotions or retelling the story in greater detail. It is about helping the nervous system complete what was once impossible: restoring regulation, releasing trapped survival energy, and relearning that safety and responsiveness are possible now.
Trauma is not intensity. It is unfinished survival — and the body remembering how it had to cope when there was no other choice.
Why You Keep Reacting Like That: How Memory and Emotion Get Stuck—and How to Heal
Have you ever found yourself overreacting to something small, only to realize later that it reminded you of something bigger, something painful? You're not alone. There’s a reason for this—one that neuroscience and somatic therapy help us understand deeply.

Have you ever found yourself overreacting to something small, only to realize later that it reminded you of something bigger, something painful? You're not alone. There’s a reason for this—one that neuroscience and somatic therapy help us understand deeply.
Your Brain is a Prediction Machine
Your brain is always trying to help you survive. One of the ways it does this is by using the past to predict the future. This is efficient: instead of evaluating every situation from scratch, your brain compares new experiences to old ones to figure out what to do next. This is the core of how memory works.
As neuropsychologist Mark Solms explains, the brain is organized around affective (emotional) needs, and it constantly builds mental maps to keep us safe and satisfied. In this way, memory becomes a survival tool. [Solms, The Hidden Spring, 2021]
The Problem with Trauma
But here's the issue. Not all memories are accurate or helpful. When you go through a trauma—defined not by what happened, but by your nervous system’s inability to return to balance afterward—your brain records not just the event, but the emergency coping strategies you used in the moment.
Instead of remembering a completed emotional response (like a full cry or a protective act), your nervous system may remember a stuck state—fight, flight, or freeze energy that never got to finish. According to Peter Levine, this is the hallmark of trauma: incomplete survival responses held in the body. [Levine, Waking the Tiger, 1997]
So when something in the present even vaguely resembles that traumatic past, your brain says, “I’ve seen this before—danger!” and launches the same coping pattern, even if it’s not actually needed.
How Emotion Shapes Memory
Jaak Panksepp, a pioneer in affective neuroscience, identified core emotional systems in the brain that are shared across mammals, such as FEAR, SEEKING, RAGE, and CARE. These are deeply embodied—not just ideas in your head, but powerful forces in your nervous system. [Panksepp, The Archaeology of Mind, 2012]
When trauma distorts how these emotional systems operate, it can cause you to misinterpret present situations through the lens of old pain. You might withdraw in fear during a conflict, lash out in frustration, or numb out altogether—not because of what's happening now, but because of what your body remembers.
So How Do You Change This?
Healing involves interrupting that old survival loop. Here’s how to start:
Notice what happens in your body, emotions, impulses, and thoughts when you’re triggered. This builds awareness.
Support your nervous system with tools that create safety—slowing your breath, grounding yourself, using soothing touch or movement.
Work with your body to help it finish incomplete survival responses—shaking, crying, pushing, or other instinctive actions.
Let the emotions express. When you feel safe enough, those stuck feelings can finally move and release.
Reflect gently. Ask what meaning you attached to the event—were you unsafe, unloved, powerless? Are those meanings still true today?
Revisit the present moment and see it with fresh eyes. Is this current situation truly dangerous, or is it echoing something old?
This process doesn’t usually happen all at once. It’s slow, layered, and best done in the safety of a therapy relationship. Somatic Experiencing, developed by Peter Levine, is specifically designed to help you do this in a regulated, embodied way. With the presence of a therapist, your nervous system can borrow calm from theirs—a process known as co-regulation.
Sources:
Levine, P. A. (1997). Waking the Tiger: Healing Trauma.
Panksepp, J., & Biven, L. (2012). The Archaeology of Mind: Neuroevolutionary Origins of Human Emotions.
Solms, M. (2021). The Hidden Spring: A Journey to the Source of Consciousness.
Understanding Your Body's Alert System: A Guide to Feeling Safer in Everyday Life
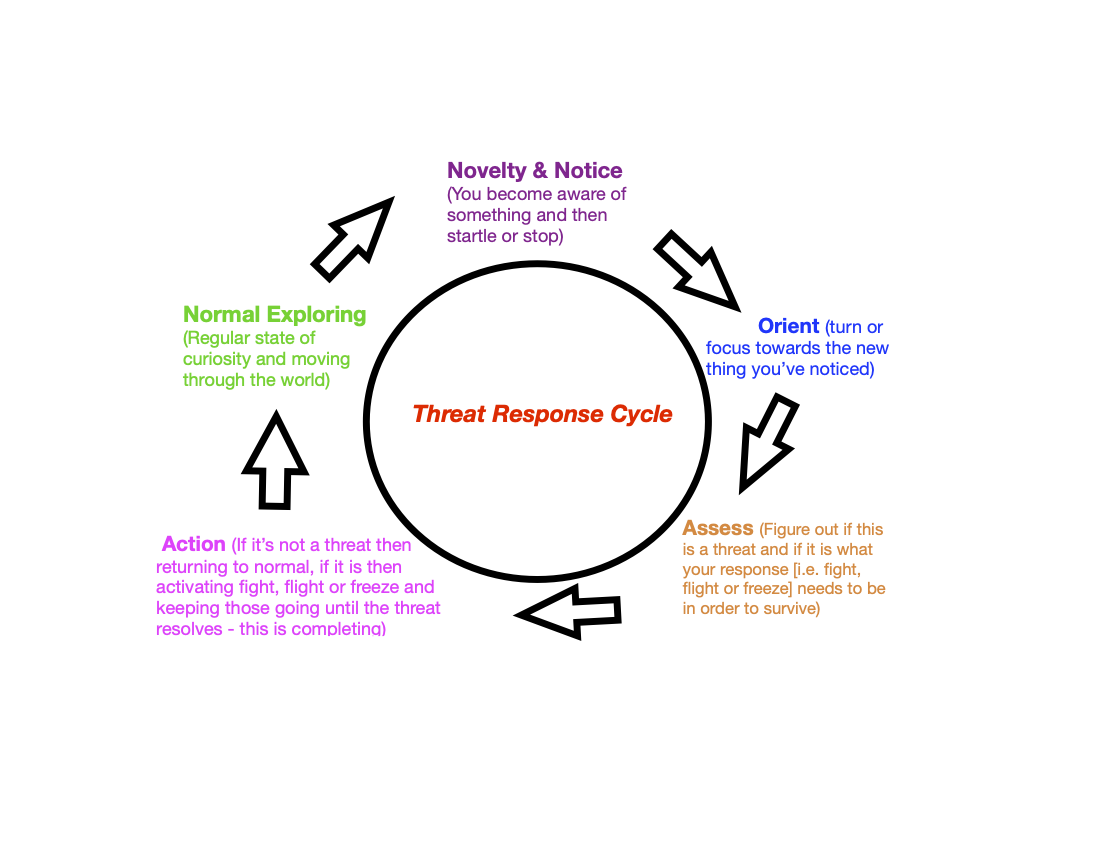
Ever notice how your body reacts when you open a stressful email or get into an argument? That racing heart, those tense shoulders - these aren't random reactions. They're part of your body's natural alert system called the threat response cycle, and understanding this system can change your life in wonderful ways.
Ever notice how your body reacts when you open a stressful email or get into an argument? That racing heart, those tense shoulders - these aren't random reactions. They're part of your body's natural alert system called the threat response cycle, and understanding this system can change your life in wonderful ways.
Your Built-In Safety System
Think of your body as having a special safety alarm, an instinct for safety. Just like our ancestors needed this alarm to stay safe from wild animals, we use it today in our modern world. This system kicks in when:
Reading a difficult email
Sitting through a tense meeting
Having a disagreement with someone you love
Walking into a crowded restaurant
Even chatting with a friend when a sensitive topic comes up
The Threat Response Cycle
Why Understanding This Matters
When you know how your alert system works, you gain a superpower: the ability to pause and check if you really need to be on high alert. Sometimes your alarm might go off when you're actually safe, like feeling panicked about giving a presentation to friendly colleagues. Other times, you might not notice real warning signs when you should, like staying in an unhealthy situation for too long.
Taking Back Control
The good news? Once you recognize when your alert system is active, you can:
Take a moment to pause
Look around and check if there's a real reason for concern
Choose how to respond rather than just react
Return to feeling calm and present when you realize you're safe
This awareness helps you move through your day with more peace and confidence. Instead of being controlled by automatic reactions, you can choose how to respond to life's challenges.
Remember: Your alert system isn't your enemy - it's trying to protect you! Learning to work with it, rather than against it, can help you feel more in control and at peace in your daily life.
Beyond Talk Therapy: Discovering Somatic Experiencing
There's a special way to help with feelings that are hard to access or even know about. It's called Somatic Experiencing.

Why We Think and Talk
We think and talk for lots of reasons. One of those reasons is to feel better. Let's explore this more.
How Thinking and Talking Help Us
When we feel something strong inside, we want to let it out. This brings us relief and contributes to our life. Here are some examples:
- When we're sad, talking to someone helps us feel less sad and understand ourselves better
- When we're angry, we might want to rant to someone about what's bothering us, think about how to solve what’s bothering us and maybe even fantasize about what we could have done differently, all in an attempt to feel less angry.
- When we do something good, we want to share it with others, this helps us feel more whole and happy.
- When we’re intrigued about something we think about what’s grabbed our attention in order to enjoy the exploration and hopefully to eventually feel the relief of understanding
Our feelings are like messages from our body. They tell us what is going on and what we need to feel better and live happier lives.
Why Some Feelings Are Hard to Notice or Talk About
Sometimes when we share our feelings, things don't go well. Maybe someone didn't listen, or we got hurt. When this happens, we might start automatically hiding these feelings, even from ourselves and even before we know we’re having them. This can make us feel worse over time. They can even cause us to misunderstand the present, to confuse our current situation with the past and react poorly because of that. With feelings that are stuck, out of our awareness and causing us problems talking and thinking alone are about the slowest ways there are to feel better. And often then only keep us stuck.
A Different Way to Feel Better
There's a special way to help with feelings that are hard to access or even know about. It's called Somatic Experiencing. Instead of just talking, we:
- Pay attention to your body and the sensations inside
- Allow some of the movements from spontaneous impulses in the body
- Learn how to navigate activation and de-activation in the body which helps you deal with stuck, pent up feelings little by little instead of in an overwhelming way.
- Empowers you
- Plus much more
Someone trained in Somatic Experiencing helps you do this safely. They teach you how to listen to your body and understand what it's telling you. While you still talk about your feelings, you also learn to feel them in a way that's comfortable and safe. This brings things that are unconscious to the light of day and lets them out so you feel better and live easier.
All of which helps you find answers that come from deep inside yourself, making you feel more sure about what you need.
Are these feelings shadows or real?
Our brains are prediction machines using the past to predict the future and un-healed past events cloud those predictions and can cause un-adaptive emotions.

Here is this post summarized in three sentences:
Our brains are prediction machines using the past to predict the future and un-healed past events cloud those predictions and can cause un-adaptive emotions.
Slowing down and reflecting using non judgement and lots of self acceptance helps us suss out whether our feelings are adaptive or not.
Working on our past helps our present be clearer.
It’s popular to say that you won’t let fear drive your life. While that’s maybe an important counter balance to living too much in fear or giving away your personal power it’s also a misnomer. The goal shouldn’t be to get rid of any core emotion, instead it should be to slow down when we are sped up and automatic so that we can listen to what we’re feeling (this might take a lot of self acceptance and be alarming to do). That is how we start to be truly adaptive. Remember what we feel is going to be based on both the present moment and your past. So it takes some time to suss out whether your intuition is adaptive emotions to the present moment or out of date feelings from the past being put on the current moment. Our brains are prediction machines. Their job is to efficiently predict what will happen based on the past. When the past is incomplete then we inaccurately predict. So in order to be more present we need to not only slow down we also need to process and complete or re-complete the past. Fear is important, without fear we would be much more vulnerable to being taken advantages of. That said, unnecessary fear keeps us small and under selling ourselves.
So to recap once again in those three sentences:
Our brains are prediction machines using the past to predict the future and un-healed past events cloud those predictions and can cause un-adaptive emotions.
Slowing down and reflecting using non judgement and lots of self acceptance helps us suss out whether our feelings are adaptive or not.
Working on our past helps our present be clearer.